

What should we know about skin cancer?
May is Skin Cancer Awareness Month, which is the best time to learn interesting details about skin cancer and its potentially life-threatening forms, diagnosis and treatment methods. Melanoma is the most aggressive and challenging among the skin cancers, along with squamous cell carcinoma and basal cell carcinoma. The number of melanoma cases is rising annually as a consequence of increased UV radiation. One of the most urgent problems facing medicine today is the availability of treatment options for complex forms of melanoma, particularly metastatic variants. Modern targeted therapy includes the use of BRAF/MEK inhibitors and immunotherapy (anti-PD1/anti-CTLA4 antibodies) and is characterized by promising results in most patients.
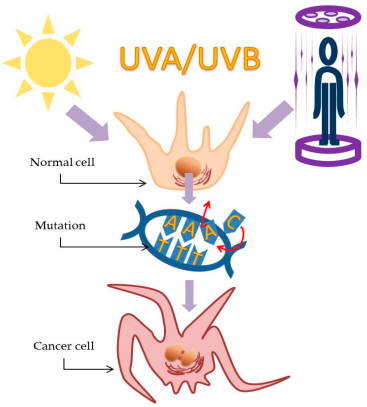
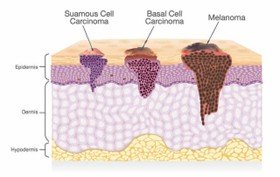
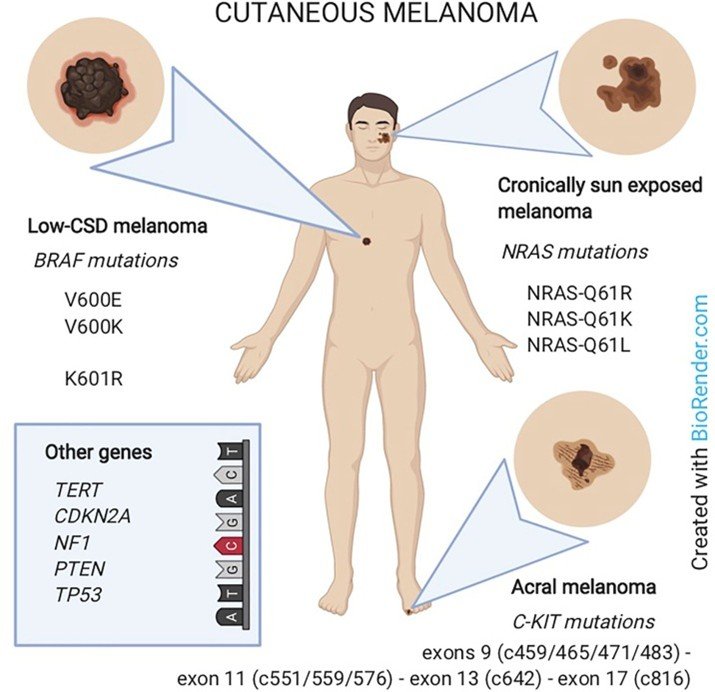
Melanoma is a malignant tumor of the pigment melanin-synthesizing cells - melanocytes. Mutation of the BRAF gene is one of its most common causes and is found in approximately 80% of cases. Among the somatic mutations that initiate various types of melanoma, mutations in the TERT, NRAS, NF1, and KIT genes are also noteworthy. Melanoma grows in two phases: radial and vertical. When melanoma tumor tissue is thin, superficial, and localized mainly in the epidermis, it is in the radial growth phase and is harmless. In the vertical growth and development phase, which may be of de novo origin or develop from radial phase lesions, melanoma cells invade deep tissues and exhibit metastatic potential. Melanoma incidence is increasing worldwide, especially in white populations with excessive sun exposure. Factors that increase the risk of developing melanoma include excessive sunbathing, use of tanning beds, changes in the number of typical moles, the presence of atypical moles, a family history of melanoma, or personal history. Traditionally, invasive cutaneous melanoma has been morphologically characterized into four subtypes: superficial spreading melanoma, nodular melanoma, lentigo malignant melanoma, and acral melanoma. It can also develop in the eye, which is called ocular melanoma. Genomic analysis has revealed the association of somatic mutation frequencies with different subtypes of melanoma. Currently, their classification according to molecular pathways of development is carried out into 9 types, and among them histological, clinical and epidemiological specificity is revealed. Melanoma lesions on the chest and extremities are induced by low-intensity UV radiation, and mutations in the BRAF gene account for 45–50% of these malignancies (molecular mechanism I). The head and neck are the primary sites of melanoma forms that arise following exposure to high-intensity UV radiation (molecular processes II–III). Upon analysis, mutations in the NRAS proto-oncogene are found in a medium frequency, accounting for roughly 10–20% of melanomas. Melanoma that develops without exposure to sunlight (methods IV-IX) is characterized by localization on the extremities and mucous membranes and does not show mutations in the BRAF, NRAS, or neurofibromin 1 (NF1) genes, although they are characterized by a relatively low frequency of mutations in the c-KIT proto-oncogene (tyrosine kinase receptor) (15%). The early phases of tumor evolution are typically triggered by mutations in the BRAF, NRAS, and NF1 genes, which cause the mitogen-activated protein kinase (MAPK) signaling pathway to be abnormally active.