May is Skin Cancer Awareness Month, an appropriate time to review the most important facts about skin cancer, its potentially life-threatening forms, and the role of modern diagnosis and treatment. Among skin malignancies, melanoma is considered the most aggressive and clinically challenging, alongside squamous cell carcinoma and basal cell carcinoma.
The global incidence of melanoma continues to rise, partly in association with increasing ultraviolet exposure. One of the most urgent issues in oncology today is the availability of effective treatment options for advanced and metastatic melanoma. Modern practice increasingly relies on targeted therapy with BRAF/MEK inhibitors and on immunotherapy with anti-PD-1 and anti-CTLA-4 antibodies, both of which have produced promising results in many patients.
What Is Melanoma?
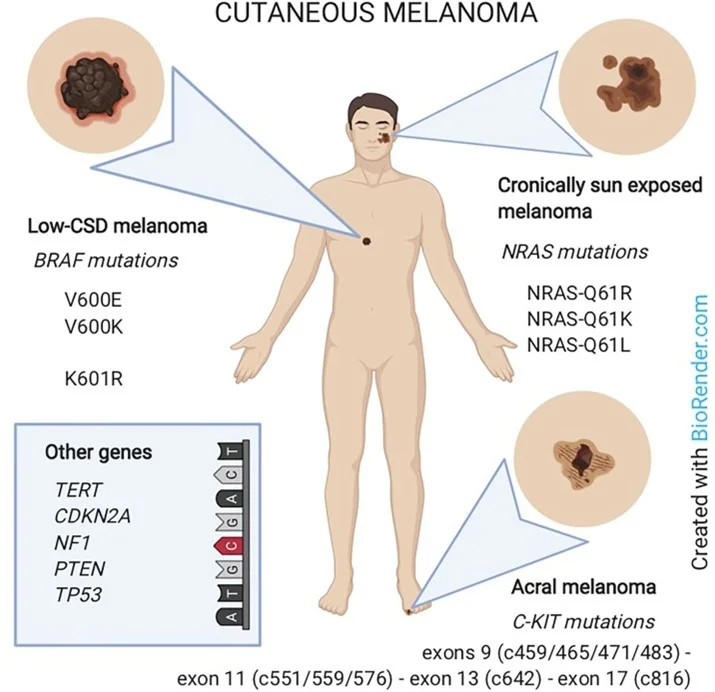
Melanoma is a malignant tumor that arises from melanocytes, the pigment-producing cells responsible for synthesizing melanin. Mutation of the BRAF gene is one of the most common drivers and is reported in a large proportion of cases. Other clinically important somatic alterations include changes in the TERT, NRAS, NF1, and KIT genes.
Melanoma develops through two broad growth phases. In the radial growth phase, the lesion is typically thin, superficial and mainly confined to the epidermis. In the vertical growth phase, melanoma cells invade deeper tissues and acquire metastatic potential. This distinction is clinically important, because invasive disease behaves very differently from a superficial lesion.
Risk Factors and Molecular Subtypes
Melanoma incidence is increasing worldwide, particularly in fair-skinned populations with high cumulative sun exposure. Important risk factors include excessive sunbathing, the use of tanning beds, changes in the number of common moles, the presence of atypical moles, a family history of melanoma, and a personal history of the disease.
Traditionally, invasive cutaneous melanoma has been divided morphologically into four major subtypes: superficial spreading melanoma, nodular melanoma, lentigo maligna melanoma, and acral melanoma. Melanoma may also arise in the eye, where it is referred to as ocular melanoma. Modern genomic analysis has shown that the frequency and pattern of somatic mutations vary across melanoma subtypes, and contemporary classification increasingly reflects molecular pathways in addition to morphology.
Melanoma arising on the trunk and extremities is often associated with lower-intensity UV exposure and shows BRAF mutations in approximately 45–50% of cases. Melanoma of the head and neck is more often associated with higher-intensity UV exposure. NRAS mutations occur at an intermediate frequency, while melanomas that arise without meaningful sun exposure—such as some acral and mucosal lesions—are less likely to harbor BRAF, NRAS or NF1 mutations, but may demonstrate KIT alterations.
At the biological level, early tumor evolution is often driven by mutations affecting the MAPK signaling pathway. This is one of the reasons molecular profiling has become an integral part of modern melanoma management.
Modern Treatment of Metastatic Melanoma
Historically, metastatic melanoma was one of the most difficult malignancies to treat. The development of targeted molecular inhibitors and immunotherapy has significantly improved outcomes over the last decade. In the past, chemotherapy—most notably dacarbazine—was considered the only systemic treatment option, but it was associated with low response rates and is now generally reserved for selected patients who do not benefit from immunotherapy or targeted therapy.
Today, immunotherapy is a first-line systemic strategy in many settings. In patients with a confirmed BRAF mutation, a combination of BRAF and MEK inhibitors can also be highly effective. For example, in patients with a BRAF V600E mutation, combining a BRAF inhibitor such as vemurafenib with a MEK inhibitor such as cobimetinib has shown better outcomes than BRAF inhibition alone.
Why Molecular Diagnostics Matters
Technologies such as next-generation sequencing (NGS) and real-time polymerase chain reaction (rtPCR) allow precise characterization of the tumor’s genetic profile. In melanoma, this information is essential for treatment planning and helps identify clinically actionable targets before therapy begins.
At NV Genetics, melanoma-related testing includes the detection of relevant target gene mutations by NGS, including BRAF, NRAS, TERT, NF1, and KIT. Detection of BRAF gene mutations by rtPCR includes highly sensitive genotyping of V600E, V600E complex, V600K, V600D, and V600R point mutations.
In practice, this means that modern melanoma care is no longer based solely on morphology. It depends on understanding the molecular biology of the tumor and selecting the most appropriate therapy for each individual patient.

